The problem of American patients not adhering to their medication as directly prescribed is a $290 billion burden to our economy. The growing cost of healthcare is increasingly in focus; it is time for patients, caregivers, payers, governments and the pharmaceutical industry to work together to reduce this waste.
With the advent of another presidential election cycle, we are caught up in a familiar debate about the cost of healthcare. Naturally, the pricing of pharmaceuticals is front and center — even more so than in previous campaign years — due to the recent media firestorm surrounding the exorbitant price increases of some generic medications. But there is another issue, one depriving the U.S. healthcare system of billions of dollars, which is not being addressed in an open forum.
This problem is poor medication adherence, which occurs when patients do not take their drugs as they are designed. It should come as no surprise that this creates tremendous waste — not only from expensive drugs going unconsumed, but also from societal costs associated with poor patient outcomes.
According to the New England Healthcare Institute (NEHI), estimates by several prominent government and nongovernmental organizations, including the World Health Organization (WHO), Centers for Disease Control (CDC) and the National Institutes for Health, medication nonadherence generates as much as $290 billion in direct — but avoidable — costs in the U.S.1 Though nonadherence contributes a third of the $750 billion that the National Academy of Medicine (NAM) estimates is the total for excess costs in healthcare, neither Republicans nor Democrats addressed this issue during the 2016 election cycle. Cost and access to healthcare remain paramount, but lawmakers are missing the opportunity to bring attention to nonadherence and propose measures to reduce this waste, which contributes to the spiraling cost of health insurance coverage.2
Healthcare Still Not Affordable
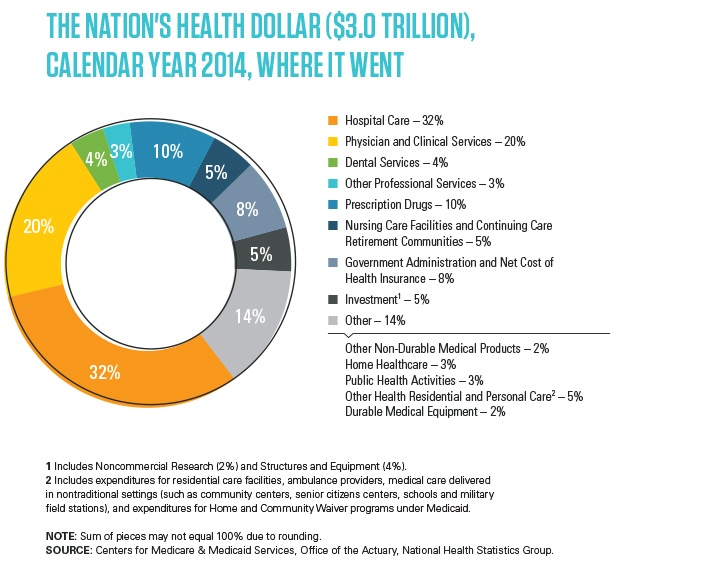
According to a 2015 report on healthcare costs, the Department of Health and Human Services’ Centers on Medicare and Medicaid Services (CMS) found “U.S. healthcare spending grew 5.3 percent in 2014, reaching $3.0 trillion or $9,523 per person. As a share of the nation’s Gross Domestic Product, health spending accounted for 17.5 percent.”3 The NAM report “Best Care at Lower Cost: The Path to Continuously Learning Health Care in America,” notes healthcare spending has increased at a greater rate than the economy for “31 of the past 40 years.”4 The growth in healthcare costs has also led to stagnation in income for America’s working-class families. The NAM explained that, even though income has increased by 30% since about 2004, the gain has been essentially wiped out by the 76% increase in healthcare costs associated with traditional modes of healthcare delivery.
Critically, the NAM report also finds that these models are generating costly unintended consequences, the result of paying clinicians and healthcare organizations to administer services and therapies “without a specific focus on patient health and value,” which has contributed to waste and inefficiency. The report concludes that these costs will surpass maintainable limits, noting: “The growth rate of healthcare expenditures is unsustainable, with waste that diverts major resources from necessary care and other priorities at every level — individual, family, community, state, and national.”
The overall contribution of drug prices to the rise of healthcare costs remains a source of ongoing debate. CDC figures from 2014 reveal prescription drug costs represent 9.8% of national health expenditures.5 Recent drug cost studies find drug prices are rising, especially among specialty drugs. Healthcare data company Truveris said prescription drug prices rose more than 10% in 2015, a number representing some $2 billion in higher costs to consumers.6 Generic drugs haven’t been immune either, with double- and triple-digit price increases for certain classes of generics or ones affected by supply disruptions. Further, it’s likely that the advent of biosimilars won’t brake biopharmaceutical prices much either, as development costs remain similar for both NMEs and biosimilars.
Some six years after its inception, it is not clear if the Affordable Care Act (as currently written) will remain law. But whatever may emerge post-Obamacare, reducing the economic burden of nonadherence must become a central focus of legislators as they consider improvements going forward.
Proper Pharmaceutical Use is Critical
The leading causes of death include heart disease, cancer, lung disease, stroke and Alzheimer’s, and according to 2012 CDC data, approximately half the population (117 million people) live with at least one chronic disease.7 Government data shows seven of the top 10 causes of death in 2010 were the result of chronic diseases, with heart disease and cancer responsible for nearly 48% of all deaths. Arthritis is the most common cause of disability; according to CDC, some 53 million U.S. adults suffer from this painful disease.
This trend toward treating increasingly elderly patients with multiple chronic conditions is not likely to abate, as many of the world’s developed and fast-developing economies increase their uptake of pharmaceuticals. Unfortunately, chronic diseases tend to have chronic costs. This includes expenses associated with the corresponding drug treatment. Payer systems are focused on managing these costs and continue to put pressure on the pharma industry to suppress drug prices, unrelated to the economics associated with developing and manufacturing pharmaceuticals or to the benefits of the drug.
“Because ongoing use of prescription medication is a key component of treatment for chronic conditions,” says Roebuck, et al., in “Medication Adherence Leads To Lower Health Care Use And Costs Despite Increased Drug Spending,” ensuring patients take drugs as prescribed for them “is a matter of great importance to policy makers, insurance plan sponsors, physicians, and patients.” Study authors confirmed that patients who adhere to their medication regimens enjoy better health outcomes and explained that compliant patients “make less use of urgent care and inpatient hospital services, compared to patients with similar medical conditions who are not adherent.”8 Regardless of the evidence, in spite of how much can be gained, the WHO reports average medication compliance rates in developed countries are just 50%.
Research and real-world experience confirms that when drugs, however effective clinically, reach consumers, their therapeutic value can be diminished dramatically — largely because they are not taken as prescribed. For instance, patients with chronic vascular disease who adhered to their medication underwent less hospitalization and emergency-department use.8 Indeed, improving medicine adherence has the best potential to cut healthcare costs in the short term.
According to the paper “Adherence and Healthcare Costs,” an increasing number of private payers are implementing “value-based insurance designs,” to encourage adherence.9 For example, “The Medicare Modernization Act” of 2003 mandated Medicare Part D prescription drug plans to include medication therapy management (MTM). MTM is intended to advance medication adherence through patient education, conducting comprehensive reviews of a patient’s drug regimens and monitoring the efficacy and safety of medication therapies.10 Also for consideration is the introduction of the ACA’s 5-Star rating system, which puts MTM in the spotlight.
Easy-access and portable containers, including single-unit dose formats, have proven to deliver a positive impact, especially with elderly patients.
Fee for Service — On its way out
As with most aspects of healthcare, a variety of financial incentives and payment models are in use. However, most of these models tend to pay clinicians and healthcare organizations without a specific focus on patient health and value, which contributes to the nonadherence issue. Most current systems pay healthcare providers in a “Fee-for-Service” (FFS) model. This means that for any service you undergo, you pay separately for what you have received.11 The argument is that this FFS model is depleting the healthcare system, as the emphasis is on volume. This translates to a cost, represented by an individual; one who is ill is actually more valuable than someone who is healthy, which can potentially result in doubling of services, unnecessary services or tolerance of nonadherence to drug regimens.
To move past FFS, public and private healthcare payers are experimenting with new provider payment models and other alternatives for care. These new models include patient-centered medical homes, accountable care organizations (ACOs) and episode-based payment plans that are designed to slow the pace of spending growth and achieve better healthcare quality. According to Health Affairs, “20 of the 33 quality measures to which Medicare ACOs are accountable are related to the safe and effective use of medications.”
A New Approach to Product Development
Perhaps no other sector of the economy has contributed more to improving the world’s health and well-being than the pharmaceutical industry. If the industry lives and breathes on quality by design, why is the crucial step of adherence by the patient often overlooked? It’s time to seek further innovation and consider the human element in formulation, with the question, “How will the product be used in the real world?” For the sake of patients and the industry, more attention must be paid to how well products perform in the hands of the users, which requires innovating across all fronts to improve the ease of use for medicines as prescribed. Fortunately, that work has already begun.
Pharmaceutical manufacturers have also responded to the social and economic factors driving the fight against poor prescription medication adherence. R&D spend is shifting away from blockbuster business models to more patient-centric product strategies that address the pharmacokinetic and pharmacodynamic characteristics of the different first-in-class, generic and OTC drugs in their portfolios. Similar to a consumer technology company studying user interfaces and device form factors, drug developers are working on drug form and dose frequency, as well as dose administration/delivery complexity to remove barriers to efficacy, mitigate patient issues post-approval and generate better patient outcomes.
The NEHI study uncovered a number of key design principles for medication-adherence interventions, including patient-centered methods using direct patient contact to tailor the overall intervention to meet patient preferences and address that person’s readiness to adhere. New England Healthcare Institute analysts also suggested forming a holistic view of the patient based on a complete understanding of the person’s medical condition, as well as full accounting of all their prescriptions. It is at this intersection that physicians, pharmacists and caregivers can all play a primary role in intervening with patients to improve their adherence and better outcomes overall.12
Simplifying medication dosing regimens and improving a given medication’s relative ease of use is now well understood to be primary strategies for improving adherence behavior. Combination therapies or new/alternative therapies that treat multiple conditions can help ease dose frequency or dose complexity. Extended-release formulations can have a similar impact, reducing dose frequency because one dose lasts longer.
Packaging can also play an effective role in supporting adherence. Easy-access and portable containers, including single-unit dose formats, have proven to deliver a positive impact, especially with elderly patients. Unit-dose medication delivery is popular both in the U.S. and Europe because it helps prevent under- and overdosing and similar medication errors. This is especially true for elderly or impaired patients who may have trouble navigating medication regimens across several multiple-dose packages. Single-dose packaging helps accurately administer drugs and therapies because they hold only a single dose of a drug and are meant to open only once.
Most dosage forms can be packaged as unit doses, including oral, topical and parenterals. Blister and pouch packaging for OSDs are common, as are pre-filled syringes and cartridges for parenterals. Squeeze tubes and blow-fill-seal containers effectively deliver topical, oral and sterile formulas, such as ophthalmic and respiratory agents.An open, honest and transparent relationship is what i think will ensure long-term success between two organizations versus one trying to win.Development, Education and Collaboration
The need to improve medication adherence is abundantly clear, and the answers are becoming so. Study after study confirms that the closer the industry gets to the patient the better; health outcomes improve and so does the cost profile to payers. The pharma industry is being compelled to demonstrate its social value even more strongly than ever before. Rather than waiting for legislation or market forces to act, the industry must be proactive to better serve their ultimate customers — the patients — by collaborating closely to drive initiatives across three broad fronts:
- Increased investment and innovation to design and deliver therapeutically efficient, patient-centric products that are easier to use safely and correctly in the real world.
- Comprehensive consumer education programs to drive medication adherence, with pre- and post-approval studies to determine why failures occur.
- Collaboration among stakeholders (manufacturers, regulators, academia, providers, payers, patient advocates and governments) to institute models that reward therapeutic efficiency and value outcomes, rather than services delivered.
Technologies that support easy-to-use dosage and packaging forms are readily available; CDMOs like Unither Pharmaceuticals have been introducing successful solutions to the industry for years. Unither offers a comprehensive range of single-use dosage forms and delivery systems that help mitigate adherence issues and support effective patient-centric therapies. These forms are proven to be a convenient, affordable way for patients to consume single doses of liquid and semi-liquid medicines, as well as patient-friendly respiratory and orally digestible dose formulations. These and other innovations allow Unither to support its customers’ patient-centric drug development plans, including the shared goal of combatting poor drug compliance.
It is imperative that the healthcare industry, payers and governments act deliberately to address this multi-dimensional and highly complex issue. Better medication adherence saves lives and has the potential to cut billions of dollars in waste from the system. Although it is likely the current structure of U.S. health insurance policy and law will change, its final form has yet to be determined and may be years away. Regardless, all stakeholders need to take bold steps, both to ensure this critical aspect of healthcare policy is not ignored and that valuable pharmaceuticals are taken as intended to deliver the best outcomes for patients.
Conclusion
Accelerating process development activities is crucial for remaining competitive in the pharmaceutical marketplace today and requires strong collaboration with analytical method development efforts. As a contract development and manufacturing organization (CDMO) dedicated to providing advanced process development capabilities, GSK Biopharmaceuticals has established a highly experienced analytical team focused on supporting process development with the specific goal of enabling the rapid scale-up and tech transfer of biopharma partner processes.
References
- Thinking Outside the Pillbox: A System-wide Approach to Improving Patient Medication Adherence for Chronic Disease. Rep. New England Healthcare Institute. Aug. 2009. Web.
- Transformation of Health System Needed to Improve Care and Reduce Costs. The National Academies. 6 Sept. 2012. Web.
- “National Health Expenditure Data.” Centers for Medicare & Medicaid Services. Web.
- Smith, Mark, Robert Saunders, Leigh Stuckhardt, Michael J. McGinnis. Best Care at Lower Cost: The Path to Continuously Learning Health Care in America. Rep. Institute of Medicine. 13 July 2010. Web.
- “Health Expenditures.” Centers for Disease Control and Prevention. Web.
- Americans Faced Double Digit Increases in Prescription Drug Prices in 2014, According to Truveris National Drug Index. Truveris. 26 Jan. 2015. Web.
- “Chronic Diseases: The Leading Causes of Death and Disability in the United States.” Centers for Disease Control and Prevention. Web.
- Roebuck, Christopher M., Joshua N. Liberman, Marin Gemmill-Toyama, Troyen A. Brennan. “Medication Adherence Leads To Lower Health Care Use and Costs Despite Increased Drug Spending.”Health Affairs 30.1 (2011). Web.
- Luga, Aurel O., Maura J. McGuire. “Adherence and Health Care Costs.” National Center for Biotechnology Information 7 (2014): 35-44. Web.
- Varshneya, Ashish. “Medication Non-Adherence: A $290 Billion Unnecessary Expenditure.” HealthWorksCollective. 13 Apr. 2015. Web.
- Sanghavi, Darshak, Meaghan George, Kate Samuels, Rio Hart. “The Beginner’s Guide to New Health Care Payment Models.” Brookings. 23 July 2014. Web.
- Viswanathan, Meera, Carol E. Golin, Christine D. Jones, Mahima Ashok, Susan J. Blalock, et al. “Interventions to Improve Adherence to Self-administered Medications for Chronic Diseases in the United States: A Systematic Review.” Annals of Internal Medicine 157.11 (2012): 785-795. Web.