Antisense oligonucleotide (ASO) therapies offer a new approach to disease treatment. Rather than interfere with the activity of problematic proteins, they are designed to prevent their production. Several ASO drugs have already been approved by the U.S. FDA and the EMA, and many more are progressing through clinical studies. Target diseases range from metabolic disorders and genetically driven conditions to neurodegenerative diseases. As more is learned about disease mechanisms and the chemistry and biology of ASOs, additional opportunities continue to arise, leading some to consider ASOs the third most important category of drugs, behind small molecules and biologics.
Interfering with a Fundamental Biological Pathway
The biochemistry of living beings starts with DNA, which encodes RNA molecules that are translated into proteins that perform the key reactions in the body necessary for life.1 More specifically, the DNA is transcribed into “pre-mRNA” containing introns and exons.2 The introns are removed, and the exons are spliced together to form mRNA for translation into proteins. Aberrant proteins that result when this fundamental process does not function correctly lead to many different types of diseases.
Antisense oligonucleotides (ASOs) — synthetic short, single-stranded DNA molecules comprising the four basic amino acids adenine (A), cytosine (C), guanine (G), and thymine (T) — are designed with specific sequences so that they bind via Watson–Crick base pairing to specific pre-mRNA molecules to influence (i.e., to correct aberrant or initiate missing) protein synthesis. This concept is feasible because there is a very high probability that a given RNA or DNA sequence longer than 13 and 17 nucleotides, respectively, occurs only once in the human genome.3
ASOs achieve gene silencing by impacting mature mRNA expression though inhibition (downregulation) of translation by binding with the translation initiation codon of mRNA or through induction of RNase H endonuclease activity, which results in the cleavage of the target RNA–DNA heteroduplex and hydrolytic RNA degradation. Some ASOs interfere with the formation of the mRNA 5′ cap, alter the exon splicing process, or sterically hinder ribosomal activity (steric block ASOs).1–4
Most ASOs are 10–30 nucleotides in length, negatively charged, and chemically modified in some way to prevent enzymatic degradation, improve binding affinity, solubility, and in vivo stability, and/or enable delivery to targeted tissues.4,5 Modification typically involves incorporation of non-natural nucleotides — natural nucleotides with different functional groups, such as 2′-O-methoxy-ethyl (2′-MOE) group at ribose position 3 and replacement of phosphate moieties along the nucleic acid backbone with phosphorothioate (PS). ASOs may also be conjugated to peptides, antibodies, and other biomolecules to aid targeted delivery and uptake.6
Many Attractive Features
ASOs are different from traditional small molecule and even newer biologic drugs, because they address problems associated with protein expression (over- or underproduction or production of mutated proteins) rather than the proteins themselves.3 The ability to target specific pre-mRNA through careful design typically results in a low level of side effects with ASO therapies and allows the development of highly personalized treatments addressing patient-specific mutations. In addition, ASOs make it possible to target proteins involved in disease mechanisms that were previously thought to be undruggable.
ASOs also have a relatively simple design compared with traditional biologics and are chemically synthesized rather than produced via cell culture. Furthermore, chemical modification does not interfere with the primary activity of ASOs. Thus, it is possible to highly tune their activity and formulate products for different routes of administration (e.g., subcutaneous, intravenous, topical, oral, rectal, intranasal).1,7 The ability to select the route of administration is important, because it can impact distribution, targeting, and accumulation of therapeutic ASOs.8 Direct ASO delivery is also possible, such as local delivery in the eye or intrathecal administration to avoid the blood–brain barrier.7
Other advantages of ASOs include their minimal risk of genotoxicity, the fact that they are not CYP450 substrates and thus do not generate CYP-mediated metabolites, and a lack of drug–drug interactions (DDIs) with other small molecules.7 They also tend to have mild-to-moderate toxic effects, which may include thrombocytopenia, elevated liver enzymes, and hyperglycemia, that are generally transient and easier to control than is the case for other drug classes.2
Several Generations
As researchers have learned more about the in vivo behavior of ASOs, new chemical modifications have been developed to improve their performance.5,7 First-generation products incorporate a PS backbone to increase resistance to nucleases. Second-generation ASOs have a PS backbone, as well as modified ribose sugar groups for even more enhanced nuclease resistance and greater binding affinity. GAPmers include PS nucleotides with sugar-modified nucleotides on either side. MIXmers have PS- and sugar-modified nucleotides interspaced.
Third-generation ASOs include further modifications, such as locked nucleic acids, which are created by connecting the carbons in ribose sugar groups to restrict movement and increase RNA affinity, as well as adding MOE, methyl, constrained ethyl, or other substituents, and introducing alternative backbones (e.g., phosphorodiamidate morpholino, P-ethoxy, pseudo-peptide polymer) to increase stability, degradation resistance, and target affinity and reduce toxicity.7
In some cases, however, these chemical modifications have a negative impact on the ability of ASOs to penetrate cell membranes. Formation of conjugates can help increase cellular uptake and targeting specificity.7 Molecules that are used in ASO conjugates include antibodies, receptor ligands, oligonucleotides (e.g., aptamers), and peptides. Delivery can also be enhanced by using biocompatible/biodegradable cationic polymers, such as PLA (polylactic acid), PLGA (poly(lactic co-glycolic acid)), or PEI (polyethyleneimine), liposomes and other lipidic vessels, and inorganic nanoparticles (as conjugates).7
A Number of Approved Therapies
The first ASO, fomivirsen (VitraveneTM), was approved by the FDA in 1998 for the treatment of cytomegalovirus-induced retinitis (it has since been withdrawn due to a decline in cases of the disease). The second ASO — mipomersen for the treatment of familial hypercholesterolemia — was not approved by the FDA until 2013. Nusinersen received FDA approval for the treatment of spinal muscular atrophy (SMA) in 2016. Milasen is an ASO developed and approved in 2019 (in just 10 months) for the treatment of a 6-year-old child dying from Batten’s disease.
Since 2016, there has been a marked increase in the rate at which ASOs are being developed and approved — largely attributed to the advances in chemical modifications and the improved properties of later-generation molecules. In addition to SMA, other genetic diseases addressed with ASO therapies include Duchenne muscular dystrophy (DMD) and familial amyloid polyneuropathy.
All of the approved ASOs incorporate chemical modifications to improve stability and other properties. Many are delivered intravenously, but some are injected subcutaneously or at the site of action (intravitreally or intrathecally).2
Many ASOs in Clinical Development
In March 2022, 122 clinical trials involving ASO therapies were registered. They target a wide variety of diseases, including Alzheimer’s disease (AD), amyotrophic lateral sclerosis (ALS), cancer (leukemia, lung, and prostate), cystic fibrosis, multiple sclerosis, Parkinson’s disease, Crohn’s disease, Leber congenital amaurosis, rheumatoid arthritis, other rare neurodevelopmental disorders, and infectious diseases, such as hepatitis B virus (HBV) and SARS-CoV-2.2,5 More than a handful are late-stage phase III studies.
Interest in ASO Treatments for Neurodegenerative Diseases
ASO therapies in late-stage development (or commercialized) for neurodegenerative diseases include those for spinal amyotrophy, DMD, transthyretin-related hereditary amyloidosis, porphyria, and ALS. Treatments at earlier clinical stages target Huntington's disease, synucleinopathies, and tauopathies.9
Neurodegenerative diseases can be monogenic or extremely complex. The former can be addressed with various types of gene therapy, including ASO treatment. The latter multifactorial diseases, which include AD, present a much greater challenge. Not only is the etiology complex, it progresses dynamically. No successful treatment has yet been developed, and results of clinical trials have shown that AD drugs need to be highly specific to avoid high levels of side effects, target a specific disease stage, address multiple targets, and provide highly targeted delivery. ASOs are attractive therapies because they are highly specific and can target brain mRNA and microRNA involved in different posttranscriptional regulation mechanisms.8
ASOs to treat AD are still in early stages of development. They include therapies designed to lower toxic Aβ by targeting mRNA for amyloid precursor protein or its amyloidogenic processing enzymes and miRNA-targeted ASOs that target both amyloid and tau pathology simultaneously, such as miravirsen, developed by Santaris Pharma (now part of Roche), which is in phase II.8
Potential for Tackling Autoimmune Disorders
ASOs have attracted attention as potential therapies for various autoimmune disorders, from multiple sclerosis (MS) to inflammatory bowel diseases (IBDs).
MS is another complex disease for which ASOs offer potential treatment. Much remains unknown about the disease, and most current therapies are ineffective for a significant percentage of MS patients.10 ATL1102 is a developmental second-generation ASO therapy for patients with relapsing–remitting MS. It is an antisense inhibitor of CD49d, a subunit of VLA-4 (very late antigen-4). In a phase IIa clinical trial, ATL1102 was shown to significantly reduce the active and gadolinium-enhancing T1 brain lesions in MS patients compared with the control after 8 weeks.10,11 The drug prevents immune cells from entering the brain and spinal cord and thus causing damage. The FDA places a partial restriction on a larger phase IIb trial in 2017, and no further updates have been provided by developer Antisense Therapeutics.10 The company is currently developing ATL1102 as a treatment for DMD.
Separately, Autoimmunity Biologic Solutions, Inc., is developing an ASO targeting the interleukin 7 receptor (IL7R) gene, which encodes a cell surface receptor in T cells that plays a central role in their homeostasis.12 The company previously showed that the genetic variant rs6897932 within exon 6 of IL7R is strongly associated with increased MS risk. Its splicing/modulating ASO therapy corrects splicing of IL7R exon 6 and restores normal expression of IL7R protein isoforms in preclinical models.
IBDs, which are chronic, immune-mediated diseases of the gastro-intestinal tract, result in part from the recruitment of immune cells from the peripheral blood to the intestine.1 In many IBD patients, enhanced expression of ICAM-1, a transmembrane glycoprotein constitutively expressed on the surface of intestinal epithelial cells and vascular endothelial cells, occurs. ASO treatment (alicaforsen, ISIS 2302) in mouse models was shown to be effective, but, in clinical trials, patients saw no or unsustainable benefit when the therapy was delivered intravenously, subcutaneously, or via an enema — likely because ICAM-1 is just one mechanism of the disease.
Several other ASOs are in development to treat IBDs, including those that target NF-κB, a transcription factor comprising two proteins (p50 and p65) that regulates the expression of many inflammatory and anti-inflammatory genes, and Smad7, which affects TGF-β1 inflammatory responses.1 More work must be done to determine why preclinical success has not been realized in large human trials. Route of administration is a key factor to consider, as systemic administration may not allow for delivery of optimal concentrations of ASO therapies at the site of action.
Targeting Cancer with Liposomal Delivery
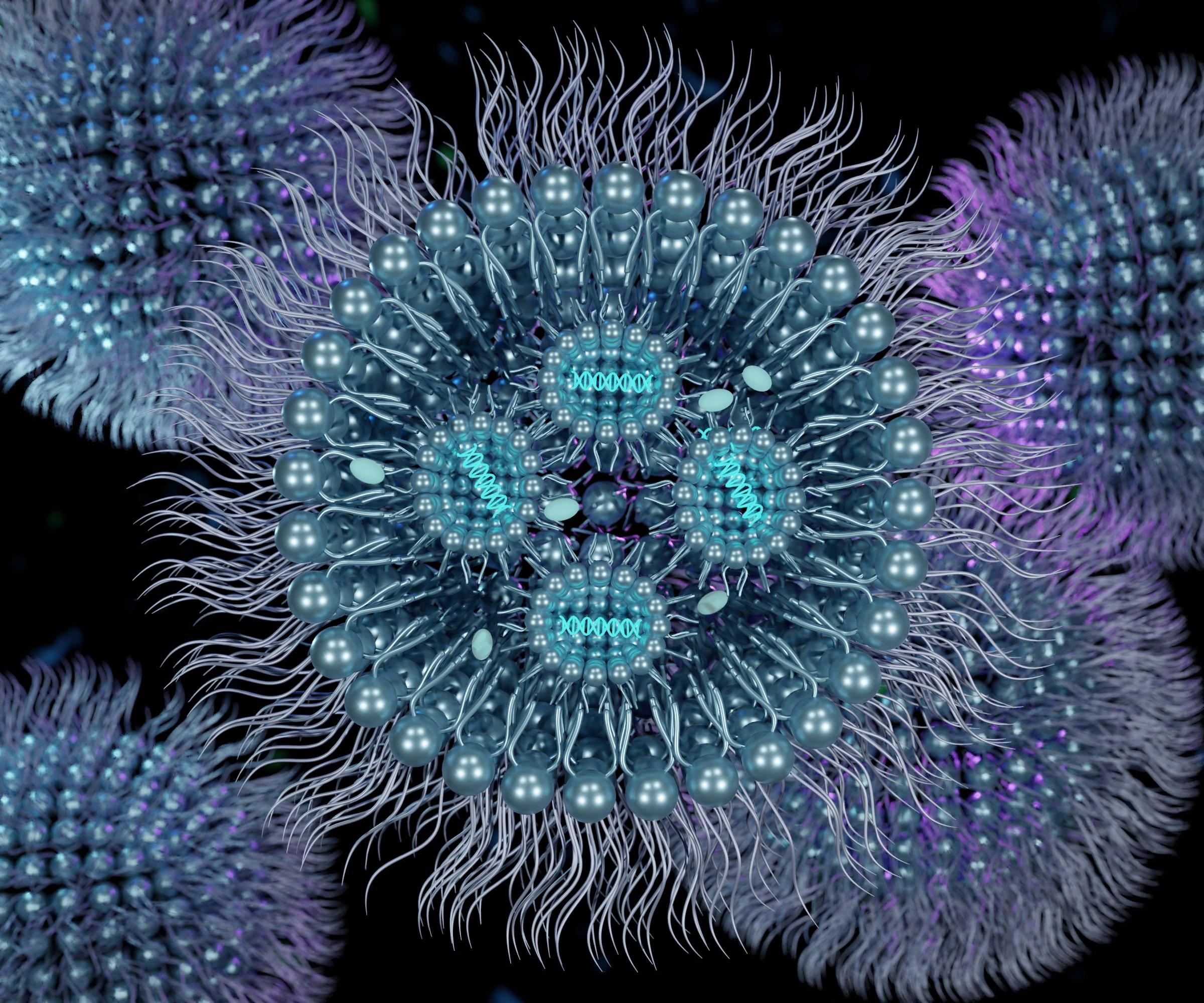
One approach to increasing the targeting ability of ASOs and their cellular uptake involves the use of liposomes as delivery vehicles.6 Liposomes have been shown to improve ASO stability, as well as enhance in vivo distribution and cellular uptake and reduce enzymatic degradation. Newer liposomes are designed to release their ASO cargos in response to specific stimuli.
The lipid bilayer in liposomes encapsulate ASOs formulated in aqueous solutions. These lipid nanoparticles are covalently attached to polymers, such as poly(ethylene glycol) (PEG), to reduce interactions with proteins and immunogenicity. They can also be conjugated to targeting moieties, such as peptides, aptamers, or antibodies. The result is improved stability, biocompatibility, extended circulation time, controlled release, and efficacy.6
Several liposomal ASOs are in clinical development. One example is BP1001 (Liposomal P-Ethoxy-Grb2 ASO) from Bio-Path Holdings, Inc. This liposome-incorporated ASO therapy targets growth factor receptor–bound protein-2 (Grb2) and is intended for the treatment of various blood cancers. Grb2 is a ubiquitously expressed adaptor protein that links activated growth factor receptors to various downstream oncogenic signaling pathways involved in cell growth, proliferation, and metabolism.6 A phase I clinical trial of BP1001 demonstrated its safety in adult patients with refractory/relapsed acute myeloid leukemia (AML), chronic myelogenous leukemia (CML), acute lymphoid leukemia, or myelodysplastic syndrome. In addition, eight doses of the investigational drug reduced the number of peripheral blood blasts in 33% of patients and bone marrow blasts in 10% of patients by at least 50%.
Future Directions
While significant improvements in ASO therapies have been achieved with the sequential introduction of new chemical medications that impact many performance aspects, challenges to the use of ASOs as therapeutic agents still remain.
For central nervous system diseases, because current ASOs cannot cross the blood–brain barrier, intrathecal injection to cerebrospinal fluid (CSF) is required, which can be risky.5 Targeting of appropriate cells is also impacted by the route of administration, and systemic delivery may not be optimal. Fortunately, other approaches, such as topical applications and enema preparations, are providing promising results.2
Better understanding of the mechanism of endosomal/lysosomal escape is needed to enable the development of novel chemical modifications and improved delivery vehicles.7 New conjugates should also allow for both improved targeting and cellular uptake. Novel lipid and polymeric nanoparticles, spherical nucleic acids, and exosomes also have potential in this regard.7
It is anticipated that artificial intelligence, advanced computer modeling, machine learning, and other novel digital tools and technologies will accelerate the development of more highly targeted and efficacious ASO therapies.7 Such advances will be needed before ASO treatments for more prevalent diseases and disorders can be realized, as underscored by the recent failure of ASO therapy for Huntington’s disease and the observed issues with long-term preclinical toxicity in multiple system atrophy and cystic fibrosis.9
Despite the challenges with ASOs, several new treatments have received marketing authorization in the last few years, and several more are in late-stage clinical trials with strong promise for success. As a result, ASOs are considered by some to be in a separate drug category following small molecules and traditional biologics,2 a designation that may increase in prominence if current treatments in the pipeline can realize their therapeutic promise.
References
- Di Fusco, Davide et al. “Antisense Oligonucleotide: Basic Concepts and Therapeutic Application in Inflammatory Bowel Disease.” Pharmacol. 29 Mar. 2019.
- Henly, Hilary. “Antisense Oligonucleotides: Improving Future Outcomes for Chronic Disease and Disorders.” Reinsurance Group of America. 15 Mar. 2022.
- Ionis Pharmaceuticals. https://www.ionispharma.com/ionis-innovation/antisense-technology/
- Hill, S.F. and H. Meisler. “Antisense Oligonucleotide Therapy for Neurodevelopmental Disorders.” Dev. Neurosci. 43:247–252 (2021).
- Kilanowska, Anna and Sylwia Studzińska. “In vivo and in vitro studies of antisense oligonucleotides – a review.” RSC Advances. Issue 57. 2020.
- Gagliardi, M. and A.T. Ashizawa. “The Challenges and Strategies of Antisense Oligonucleotide Drug Delivery.” Biomedicines. 9:433 (2021).
- Shadid, Mohammad, Mohamed Badawi, and Abedelnasser Abulrob. “Antisense oligonucleotides: absorption, distribution, metabolism, and excretion.” Expert Opinion on Drug Metabolism & Toxicology 17 (2021).
- Grabowska-Pyrzewicz, Wioleta, Andrew Want, Jerzy Leszek, and Urszula Wojda. “Antisense oligonucleotides for Alzheimer's disease therapy: from the mRNA to miRNA paradigm.” The Lancet. 74: 103691 (2021).
- Brunet de Courssou, Jean-Baptiste et al. “Antisense therapies in neurological diseases.” Brain. 145: 816–831 (2022).
- Lai, Ryner. “The Growing Role of Antisense Oligonucleotides in MS Treatment.” 7 Dec. 2021.
- Carvalho, “ATL1102 for Multiple Sclerosis.” Multiple Sclerosis News Today. 13 Jun. 2022.
- Galraza-Munoz, Gaddiel. “Novel accurate therapy for Multiple Sclerosis: Optimization of antisense oligonucleotides delivery and functionality in primary T cells.” Grantome. 2019.